Gastrectomia Billroth I e II Enfermagem Ilustrada
BY REEJA RASHEED REEJA RASHEED 2002 BATCH 2002
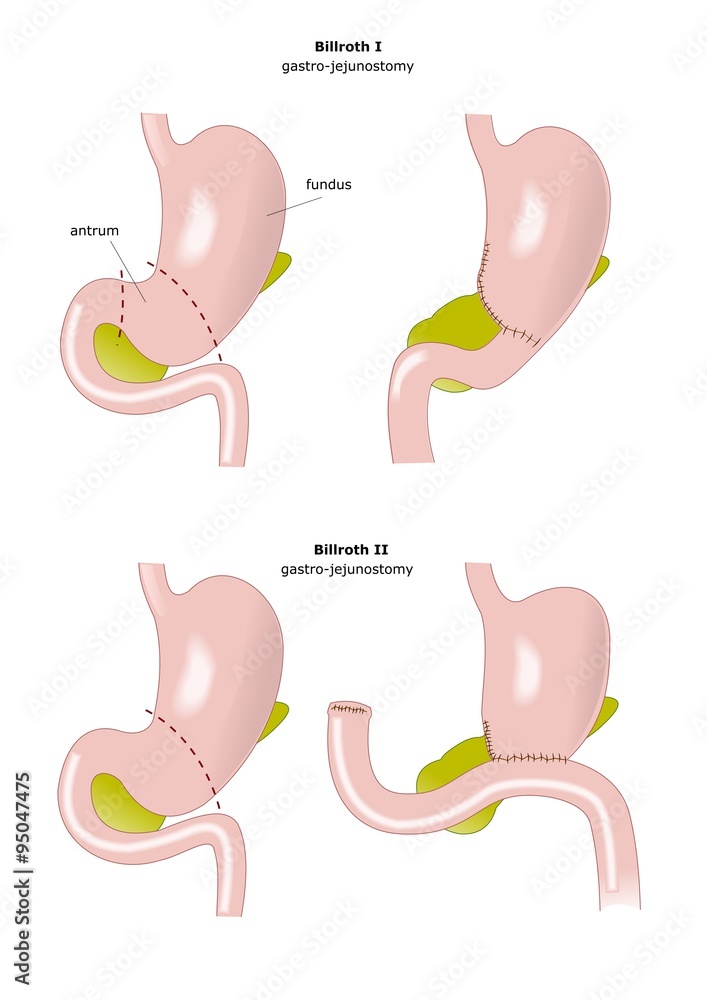
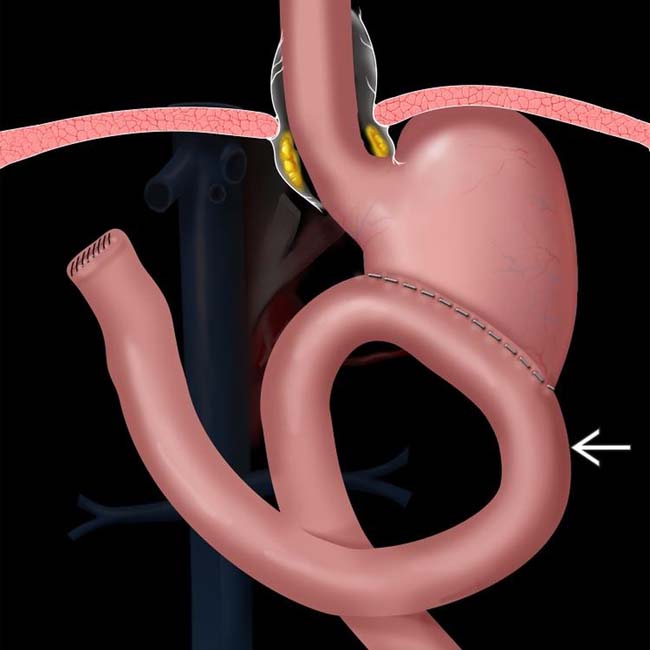
Billroth II, more formally Billroth's operation II, is an operation in which a partial gastrectomy (removal of the stomach) is performed and the cut end of the stomach is closed. The greater curvature of the stomach (not involved with the previous closure of the stomach) is then connected to the first part of the jejunum in end-to-side anastomosis.

vector illustration of scheme of resection of the stomach Billroth 2 Stock Vector Image & Art
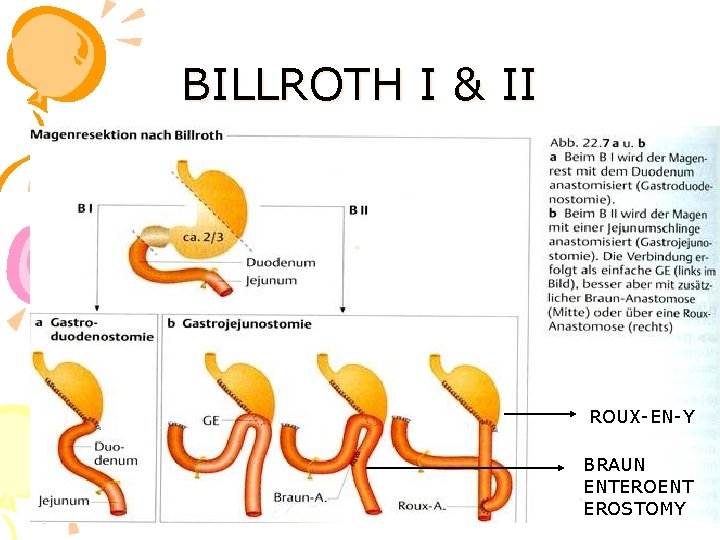
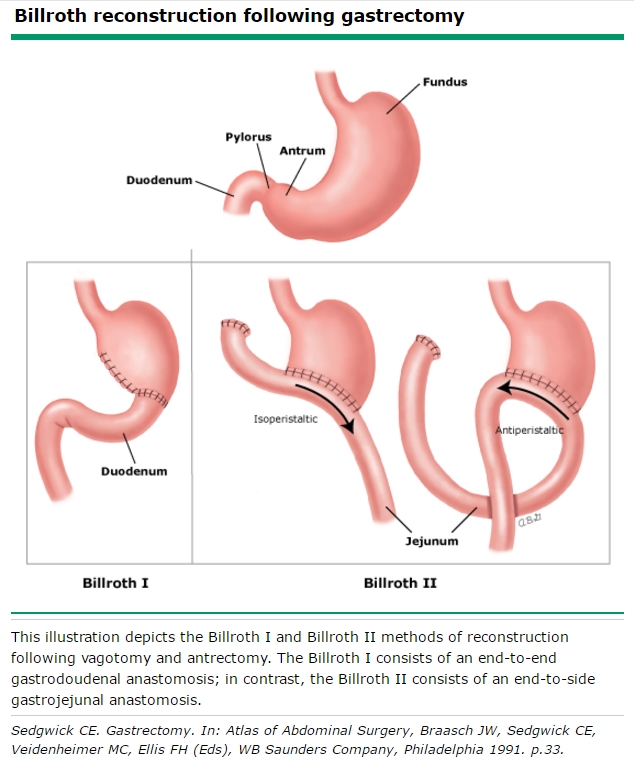
The Billroth I (BI) operation is a gastroduodenostomy that can be performed end-to-end or end-to-side. In the Billroth II (BII) reconstruction the gastrojejunostomy is performed end-to-side. As an alternative, Roux-Y (RY) reconstructions can be done (see Chapter 82 ).

SurgicalCORE Table/Figure
Therefore, we conclude that the Billroth I method should be the first choice after a distal gastrectomy as long as the anatomic and oncological environment of an individual patient allows us to perform it. However more prospective studies should be designed to compare the overall surgical outcomes of both anastomosis methods. Go to: Background
Gastrectomy Canadian Gastric Cancer Association
SUBTOTAL GASTRECTOMY: BILLROTH I AND II Step 1: Surgical Anatomy ♦ The arterial blood supply to the stomach is rich and comes from multiple sources.
resezione parziale dello stomaco secondo Billroth vector de Stock Adobe Stock
Both Billroth I and Billroth II techniques are feasible and safe reconstruction methods after LADG for gastric cancer. To reduce major complication rates, surgeons should pay attention to bleeding in Billroth I reconstruction and stump leakage in Billroth II reconstruction. Adenocarcinoma / pathology Adenocarcinoma / surgery* Gastrectomy / methods*
SurgicalCORE Table/Figure
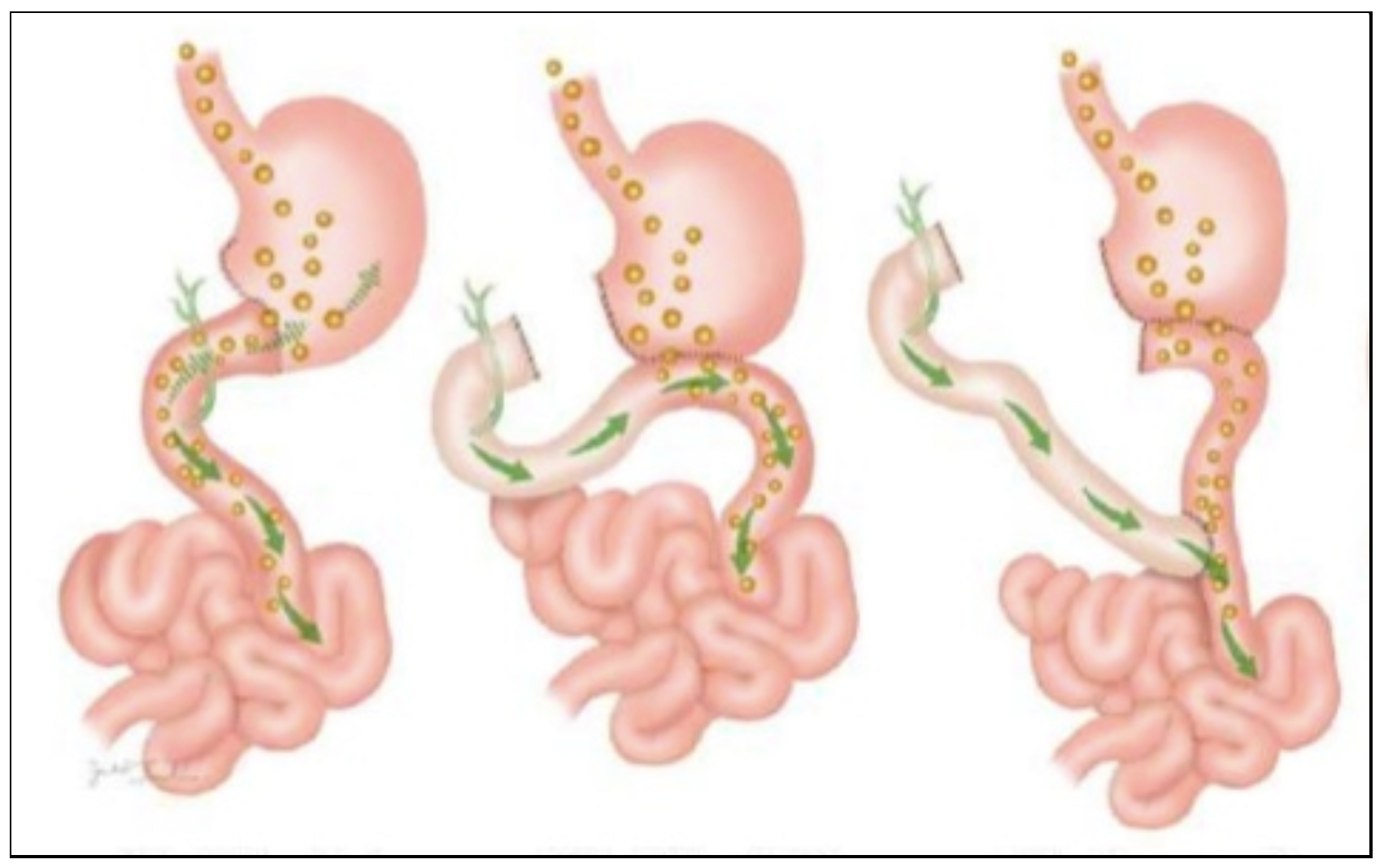
BACKGROUND/AIMS: After a distal resection of the stomach, the continuity of the gastrointestinal tract can be restored by either a gastroduodenal anastomosis (Billroth I), a gastrojejunal anastomosis (Billroth II) or a Roux-en-Y gastrojejunostomy. There is still no consensus on the reconstruction technique of choice.

Gastroenterology Education and CPD for trainees and specialists » Surgery for peptic ulcer
Gastrectomy* / adverse effects Gastroenterostomy Network Meta-Analysis Postoperative Complications* / epidemiology Randomized Controlled Trials as Topic Major surgical treatment for distal gastric cancer include Billroth I (BI), Billroth II (BII), and Roux-en-Y (RY).

Gastrectomia billroth 1 y 2
Delta-shaped Billroth I anastomosis in totally laparoscopic distal gastrectomy for digestive tract reconstruction is simple and easy to perform, and has an advantage in postoperative gastrointestinal function recovery. RY reconstruction is superior to Billroth I and Billroth II in terms of postoperative complications.
위십이지장문합술, 위공장문합술, 빌로스 I, 빌로스 II, Billroth I and II reconstruction following gastrectomy 네이버 블로그
Revisiting Laparoscopic Reconstruction for Billroth 1 Versus Billroth 2 Versus Roux-en-Y After Distal Gastrectomy: A Systematic Review and Meta-Analysis in the Modern Era World J Surg. 2019 Jun;43. 2 Department of Family Medicine, Korea University College of Medicine, Seoul, Korea. 3 Division of Upper Gastrointestinal Surgery,.
Partial Gastrectomy Bilroth Procedures Radiology Key
Background In this modern era, laparoscopic distal gastrectomy (LDG) has largely replaced open distal gastrectomy for the treatment of gastric cancer; however, a quantitative review of reconstruction methods applied exclusively using LDG has not yet been published. Thereafter, we compared three reconstruction methods (Billroth I, Billroth II, and Roux-en Y) using the data derived solely from.

Billroth I versus Billroth II Medizin, Wissen
Billroth I (B-I), Billroth II (B-II), and Roux-en-Y (R-Y) are the major reconstruction procedures after distal gastrectomy. In our study, we aimed to evaluate the functional recovery following the B-I, B-II, and R-Y reconstructions through a network meta-analysis. PubMed, Embase, and Cochrane Library databases were searched until April 2018.
PPT Cerrahpaşa Tıp Fakültesi Gastroenteroloji Bilim Dalı PowerPoint Presentation ID3372617
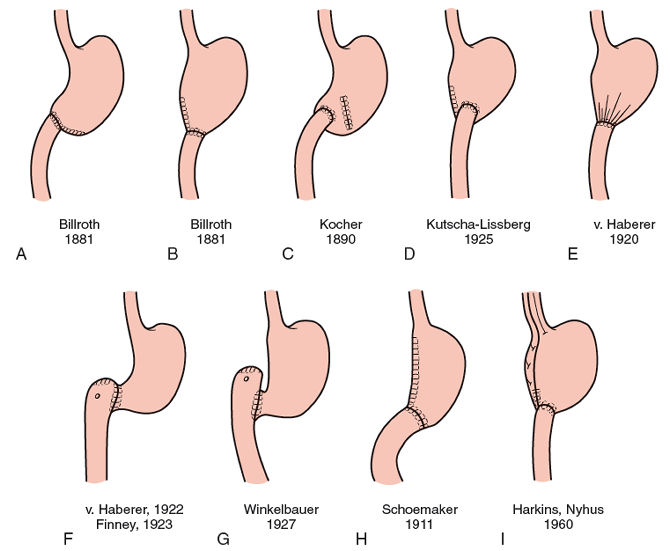
The Billroth I procedure requires extensive mobilization of the gastric pouch as well as the duodenum. This mobilization should include an extensive Kocher maneuver for mobilization of the duodenum. In addition, the greater omentum should be detached from the transverse colon, including the region of the flexures.

Comparison Between BillrothII with Braun and RouxenY Reconstruction After Laparoscopic Distal
This is one of our Complementary Videos from our Surgery Basics in 4D, 2nd Edition; with Multimedia Integration. Designed for medical students to be the Bes.

Gastrectomia billroth 1 y 2
How the intervention might work. Billroth I reconstruction may have a physiologic advantage of letting food pass through the duodenum (Kalmar 2006), and could be potentially better in reducing postoperative weight loss (Terashima 2014).However, based on the findings of an observational study, Roux‐en‐Y reconstruction has proven superiority over Billroth I and Billroth II and may be.

PostSurgical Anatomy and ERCP Techniques in Gastrointestinal Endoscopy
Although Billroth II and Roux-en-Y procedures are the two most commonly performed types of reconstruction techniques following distal stomach resection, there is yet no consensus on which reconstruction is the best choice.

Diagram of Billroth II gastrectomy. Download Scientific Diagram
Previous studies showed that the overall rate of perforation during ERCP with normal anatomy, Roux-en-Y and Billroth II were 0.35%, 2.0-11.1%, and 5.6-7.7% respectively, illustrating the increased risk in these patients. 26,33-36 Perforations usually occur when the afferent limb is entered near the duodenojejunal flexure resulting in tear of.
